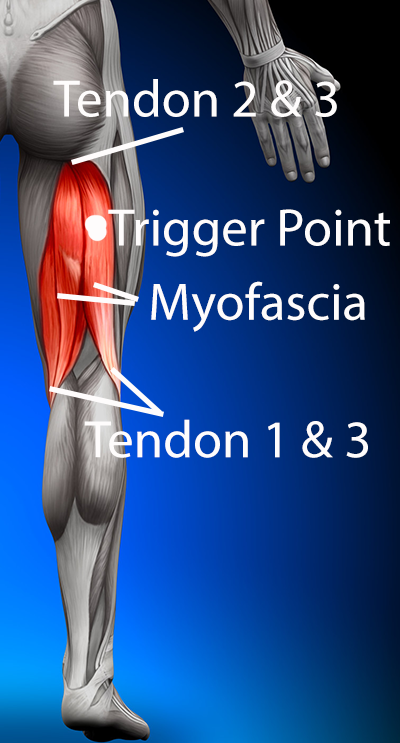
Treatment of the hamstrings often involves tendon treatment, myofascial release and trigger point therapy all using radial shockwave.
Tendon treatment is the same for the hamstring tendons as it is for any other tendon. There are lots of studies investigating the effects of shockwave therapy on tendinopathy.
There are three main reasons for using shockwave on hamstring tendons:
1. For destruction of scar tissue.
Scar tissue is destroyed due to the generation of tensile stress caused by shockwave reflections at a pressure-release boundary (Delius, 2000, Lokhandwalla & Sturtevant, 2000, Eisenmenger, 2001, Xi & Zhong, 2001, Zhu et al., 2002). Or in other words where the scar tissue and the tendon meet shockwaves create destruction. This is used mainly on the hamstring tendons at the insertional end (across the knee).

Extracorporeal shockwave to the medial hamstring tendons (semimembranosis and semitendonosis)
Machine: Gymna Shockmaster 300
Settings: 3.0bar 200 shocks at 8hz
Medium: Ultrasound Gel
2. Increased healing
At the bone tendon junction. Rompe et al. (1998) demonstrated the effects of shockwave on the Achilles tendon (in rabbits). In their study, a statistically significant increase in capillary formation was found with higher energy shock wave (0.60 mJ/mm2), which also caused more tissue reaction and potential damage to the tendon tissue. Wang, Huang & Pai et al (2002) demonstrated that shockwaves enhance neovascularization with formation of new capillary and muscularised vessels at the tendon-bone junction (in dogs). In another study, Wang et al (2003) found that shockwave therapy induces the ingrowth of neo-vessels (neovascularization) including capillary and muscularised vessels at the tendon-bone junction. As this effect often lasts over 12 weeks it is more likely this has an impact on the problem rather than the growth/proliferating factors which peak early but then return to normal levels by 8 weeks. This is the primary use of shockwave at the proximal attachment of the hamstrings where problems in the tendon tend to be at the bone tendon junction.

Extracorporeal shockwave to the hamstring origin (ischial tuberosity)
Machine: Gymna Shockmaster 300
Settings: 3.0bar 2000 shocks at 10hz
Medium: Ultrasound Gel
3. Increased healing.
This can be sub categorised into chronic and acute.
- Chronic: Wang et al. (2007) and later Wang (2012) described shockwave as having a primary treatment effect on chronic tendinopathy when the chronic tendonitis is created by an overuse syndrome. When there is pain/tenderness due to mucoid and chondroid degeneration, formation of plump tenocytes, increased fibroblastic and myofibroblastic cells and absent inflammatory cells, shockwave will have a positive impact on the area. Several studies have reported that chronic painful tendinopathies have increased numbers of sprouting non-vascular sensory, substance P-positive nerve fibres and decreased occurrence of vascular sympathetic nerve fibres. It is suggested that the altered sensory-sympathetic innervation may play a role in the pathogenesis of tendinopathy (Lian et al., 2006).
- Acute: Shockwave interferes with the serum levels of substance P and CGRP (see above). Both of these substances act on target cells in the periphery such as mast cells, immune cells and vascular smooth muscle cells, producing heat, swelling, redness and improved healing rate. (Zimmerman et al, 2009, Maier et al., 2003)

Extracorporeal shockwave to the hamstring tendons (semimembranosis and semitendonosis) at the knee for increased healing rate
Machine: Gymna Shockmaster 300
Settings: 2.0bar 2000 shocks at 12hz
Medium: Ultrasound Gel
Myofascial release to the hamstrings and trigger point therapy are often done together as these are frequently found to be dysfunctional together. However, we will look at the theory separately.
Trigger point:
Muscle treatments with shock waves (focused) was first seen in the 1990s (Kraus et al, 1999, Lohse-Busch et al, 1997). It was used as an alternative to manual trigger point treatment. The results of these treatments was reduction in pain, lower muscle tone and decreased muscle shortening.
Trigger point treatment can be separated into two areas:
- Permanently eliminate the trigger point complex. Shockwave trigger point therapy uses the concept of mechanical energy separating the fixed actin-myosin links (Travel & Simons, 1983), breaking of contraction ‘knots’ (Mense & Simons, 2001), improvement in local blood circulation through reactive hyperaemia and resolution of the ischaemia-induced energy crisis (Sikdar et al, 2010).
- Alleviate pain through reduced concentration of vasoneuroactive substances (Shah et al, 2008) as well as muscle relaxation.

Extracorporeal shockwave to the hamstring muscle (biceps femoris) for trigger points
Machine: Gymna Shockmaster 300
Settings: 2.0bar 200 shocks per point at 10hz for multiple spots (as many as required to cover the trigger points)
Medium: Ultrasound Gel
Myofascia:
Shockwave moved into the treatment of myofascial syndromes in the 2000s. Initially, radial shock waves (r-ESWT) were used for myofascial problems (Bauermeister, 2003, Gleitz, 2003), but focused shock waves followed (Bauermeister, 2005, Bauermeister, 2007, Gleitz et al, 2006, Muller-Ehrenberg, 2005). Fascia is a thin, tough, elastic type of connective tissue that wraps most structures within the human body, including muscle. Fascia supports and protects these structures. Osteopaths believe this soft tissue can become restricted due to psychogenic disease, overuse, trauma, infectious agents, or inactivity. This can result in pain, muscle tension, and corresponding diminished blood flow. Although fascia and it’s corresponding muscle are the main targets of myofascial release, other tissue may be addressed as well, including other connective tissue (DiGiovanna, Schiowitz, and Dowling, 2005).

Shockwave has been shown to be effective in muscular treatments through various mechanisms. Studies have shown separation of fixed actin-myosin links by the input of mechanical energy (spalling) as long as the force is perpendicular to the muscle fibre direction (Shah et al, 2008, Travell & Simons, 1983).
Shockwave works as a direct myofascial release method and is used to engage the myofascial tissue “restrictive barrier” (tension). Direct release is achieved with shockwave as it can mechanically influence muscles. The physiological intrinsic oscillations of 15 to 30 Hz have been described by Nazarov & Gorozhani (1988) as important for muscular relaxation, blood circulation and lymphatic drainage. Travell & Simons (1983) and Shah et al. (2008) said these oscillations could led to breaking of actin-myosin links, whilst Mense & Simons (2001) said shockwave could lead to the destruction of damaged fibers. All of which should reduce myofascial tension.
Circulatory effects e.g. improvement of blood circulation through reactive hyperaemia and angioneogenesis (Shah et al, 2008, Kuo et al, 2009, Wang, 2003) and dilution of vasoneuroactive substances as a result of reactive hyperaemia (Shah et al, 2008, Mense & Simons, 2001).
Improvements in pain through pain modulation by the release of substance P (Hausdorf et al, 2008, Maier et al, 2003) and CGRP (Takahashi et al, 2003), release and synthesis of nitric oxide (Mariotto et al, 2009, Neuland, Duchstein & Mei, 2004), selective degeneration of C-fibres (Hausdorf et al, 2008), decreases due to the pain gate control theory (Gregor & Zimmerman, 1972, Wall & Cronly-Dillon, 1960).
Reduction in muscle tone through biological mechanotransduction (Ingber, 2006, Jaalouk & Lammerding, 2009, Neuland, Duchstein & Mei, 2004).
Extracorporeal shockwave to the hamstrings
Machine: Gymna Shockmaster 300
Settings Myofascial Release: 1.6bar 3000 shocks at 16hz
Medium: Ultrasound Gel