Cellulite (medical name gynoid lipodystrophy) is found in 85% of post-adolescent women (Rossi & Vergnanini 2000, Avram 2004, Khan et al. 2010, de la Casa Almeida 2013).

Cellulite is normally categorised into 3 grades (4 if you include no cellulite). The grades are important as several studies have shown patients can normally be improved by 1 grade (Schlaudraff et al 2014). The grades are (grade 0 is no dimpling even with pressure applied):
- Dimpling when pressure applied
- Dimpling visible standing but not lying down
- Dimpling visible even when lying
Extracorporeal shock wave therapy (ESWT) and radial shock wave therapy (RSWT) have been studied and shown to be safe and effective treatment options for cellulite (Sattler et al, 2008, Knobloch et al, 2013, Russe-Wilflingseder et al, 2013, Braun et al, 2005, Angehrn et al, 2007, Christ et al, 2008, Christ et al, 2008, Adatto et al, 2010, Kuhn et al, 2008).
Video showing actual treatment to grade 2 cellulite: Shockmaster 300, 35mm deactor head, 3.6 bar, 4000 shocks, 16hz
Methods of application and dosages have varied and can be seen below:
| Who | Device | Dosage | Shocks | Frequency | Number of Sessions |
| Schlaudraff et al (2014) | 36mm Deactor | 3.5–4.0 bar | 7500 per area15000 total per session | 15hz | 2xweek for 4 weeks |
| Angehrn et al (2007) | ActiVitor-Derma® | 0.018 mJ/mm2 | 4000 shocks per leg (160cm2) | 12 sessions every 3-4 days | |
| Christ et al (2008, 2008) | C-Actor | 0.25 mJ/mm2 | 3,200 shocks per leg (600cm2) | 6/8 sessions 3-4 days apart | |
| Sattler et al (2008) | D-Actor 200 & C-Actor | 2.4–3.0 bar 0.35 mJ/mm2 | 1,909 shocks per area 1,000 shocks per area | 15hz | 6.2 sessions 6.1 sessions |
| Adatto et al (2010) | D-Actor 200 | 2.6–3.6 bar | 3000 per area | 15hz | 6 sessions over 4 weeks |
| Russe-Wilflingseder et al (2013) | D-Actor 200 | 2–3 bar then 3–5 bar | 1000 shocks (15mm head) 2500 (D20-s head) | 8 sessions 1xweekly |
It appears the most popular head is the 20mm deactor head (from Stortz). Pressures are usually higher 3+bar (180mj) and frequency is high (15hz most popular). Shocks are related to area treated i.e. back of leg 2000 shocks, buttock another 2000 shocks and on and on. Sessions are usually 2 x week for at least 6 sessions, often more (8 average).
Cellulite is normally found across large areas and no one treatment head can do the whole area in one go. To address this you will often see the term homogeneously used (Schlaudraff et al 2014). This means they moved the treatment head during the treatment to give an even number of shocks to each area. In reality this is easier said than done and so several different methods for applying the treatment have been used in the literature.
1. A common method used in practice is to simply start near one end of the treatment area then push the head towards the other end, as can be seen in this example on the thigh. Once at the end stop the shockwave, lift off, return to the start and go again. An advantage of this method on the back of the leg or thigh is the ability to push towards the lymph nodes, like cellulite massage.

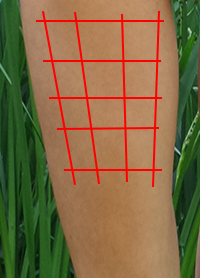
2. Create a grid (you can imagine a grid as you will leave red areas after each bout of shocks) on the area to be treated and give a fixed number of shocks in each area (Angehrn et al, 2007 used this method). This has the advantage of being very scientific but the disadvantage of potential lines in the cellulite after 3/4 sessions (we have experienced these lines). You will then need to ‘iron out’ the missed areas between the grid. This method works well if one spot of cellulite is very pronounced; you can give 200 shocks around the spot and angle the head into it during the shocks.
3. This is the most popular method in the literature. You go in a ‘snaking’ pattern one way and then the opposite way for an even numbers of shocks. This gives the most even results overall.
first snake up for 1000 shocks

then snake across for 1000 shocks

Video showing different patterns of treatment
This is a before and after picture of the left thigh and buttock following 8 sessions of radial shockwave using the Gymna Shockmaster 300, with a 35mm deactor head, at 3.6 bar, 4000 shocks per session, 8 sessions in total, at 2 sessions per week. Results after 4 weeks:

Cellulite usually develops in different people in different areas, most commonly the thighs, buttocks, abdomen and upper arms, and if well enough developed becomes visible (often referred to as “orange peel” in appearance). Cellulite is characterised by an irregular, dimpled skin surface with thinning of the epidermis/dermis and the presence of nodular clusters of fat cells (Rossi & Vergnanini 2000, Avram 2004, Khan et al. 2010, de la Casa Almeida 2013).
The development of cellulite is said to be related to various predisposing factors, such as biotype, heredity, ethnic background, body weight, age, hormonal changes, smoking, and genetic predisposition (Rossi & Vergnanini 2000, Avram 2004, de la Casa Almeida 2013, Emanuele et al. 2010, Stavroulaki et al. 2011).
Four main hypotheses of cellulite development have emerged:
- Different anatomical conformation of the subcutaneous tissue (altered connective tissue septae with sclerotic fibrous tissue septae responsible for ‘mattress’ appearance) in women compared with men; (Nurnberger & Muller, 1978, Rosenbaum et al, 1998)
- Changes in the biomechanical properties (skin compliance or elasticity) of epidermal and dermal tissues; (Rosenbaum et al, 1998)
- Excessive hydrophilia of the extracellular matrix increasing interstitial pressure and causing oedema of the fatty tissue; (Smalls et al, 2005)
- Alterations in both microvascular and lymphatic circulation resulting in the often painful protrusion of subcutaneous adipose tissue into the lower reticular dermis, causing distinctive mattress-like surface irregularities. (Lotti et al, 1990)

However, the skin and underlying structures are likely more complex than we originally thought (Lotti et al, 1990) and each explanation could be thought of as mutually conflicting (Schlaudraff et al, 2014).
Recently inflammation has been said to contribute to the formation of cellulite (Terranova et al, 2006, Avram et al, 2005).
How does shockwave reduce cellulite?
Many articles have described potential mechanisms for shockwave to reduce cellulite. Research has suggested pressure or acoustic waves are effective in disrupting the sclerotic fibrous tissue septae responsible for much of the uneven appearance of cellulite (Siems et al 2005). However other effects have been postulated; Braun et al (2005) said the stimulation of blood and lymph circulation, increased membrane permeability, and the stimulation of the exchange of blood lipids. Angehrn et al (2007) said shockwave stimulated the metabolism of fat cells and increased expression of vascular endothelial growth factor, endothelial nitric oxide synthase, and proliferating cell nuclear antigen. Christ et al (2008) said reduced oxidative stress. Siems et al (2005) thought increased antioxidants (including ascorbic acid). Kuhn et al (2008) described induction of neocollagenogenesis and neoelastinogenesis. Ferraro et al (2012) thought increased angiogenesis and apoptosis of fat cells triggered by inflammation, and activation of C nerve fibers in the skin and release of substance P according to Schlaudraff et al (2014).
Whats in a name?
Several studies on ESWT/RSWT for cellulite have used different names for the therapy e.g. acoustic wave therapy (AWT) (Sattler et al, 2008, Russe-Wilflingseder et al, 2013, Christ et al, 2008, Adatto et al, 2010) or extracorporeal pulse activation therapy (EPAT) (Christ et al, 2008, Adatto et al, 2010).
The terms AWT and EPAT are proprietary names of the manufacturer of the devices (Storz Medical, Tägerwillen, Switzerland).
AWT is described as
“… non-medical electric and electronic apparatus and instruments for the generation and application of shock waves or pressure waves in the fields of cosmetics and beauty care”, (Trademark 3712310)
and EPAT as
“… electronic apparatus and parts of the apparatus for generating and applying pressure or shock waves for use in the fields of cosmetics and beauty care”. (Trademark 3593746)
In essence AWT, EPAT and RSWT are practically the same treatments as has been shown in several papers in the literature (Christ et al, 2008, DePace, 2011, Saxena et al, 2011).
There are many reports of successful treatment of cellulite with RSWT in the literature (Sattler et al, 2008, Russe-Wilflingseder et al, 2013, Christ et al, 2008, Christ et al, 2008, Adatto et al, 2010) most showing RSWT can improve the clinical picture by one cellulite grade on average.
Schlaudraff et al (2014) said
“… in their clinical experience, the patient’s perception of their individual cellulite grade and consequently their satisfaction with the result of treatment for cellulite varies widely from one patient to another and is truly subjective. Normally, patients with low cellulite grades are more demanding and therefore more difficult to manage in their expectations, even if there is an objectively confirmed clinical improvement.”
They confirmed this in their analysis because patient satisfaction, the most important end point of any treatment for cellulite, did not correlate with improvement. There were patients with improvement by one cellulite grade who were very satisfied, whereas other patients with the same outcome were not satisfied at all.
They went further and said
“… For the clinical setting, this observation underlines the role of the therapist, who must correctly evaluate the suitability of the candidate for a cellulite treatment and must manage the patient’s expectations accordingly.”
Actual research:
Schlaudraff et al (2014) treated fourteen Caucasian females with cellulite. Mean grade at baseline was 2.5±0.09 and mean BMI was 22.8±1.17.
Method: Radial extracorporeal shock waves using the Swiss DolorClast® device 36mm head (Electro Medical Systems, S.A., Nyon, Switzerland). Patients were treated unilaterally with 2 weekly treatments for 4 weeks, totaling eight treatments on one side only. Treatment was performed at 3.5–4.0 bar, with 15,000 impulses per session applied at 15 Hz. Impulses were homogeneously distributed over the posterior thigh and buttock area (resulting in 7,500 impulses per area).
Results: The mean cellulite grade improved from 2.5±0.09 at baseline to 1.57±0.18 after the last treatment (mean was 0.93 cellulite grades) and 1.68±0.16 at follow-up (mean was 0.82 cellulite grades). Compared with baseline, no patient’s condition worsened, the treatment was well tolerated, and no unwanted side effects were observed. No statistically significant (ie, P,0.05) correlation was found between individual values for cellulite grade at baseline, BMI, weight, height, or age. They concluded radial shock wave therapy is a safe and effective treatment option for cellulite. The individual clinical outcome cannot be predicted by the patient’s individual cellulite grade at baseline, BMI, weight, height, or age.
Braun et al (2005) treated 20 patients with severe cellulite using an electromagnetic DermaSelect® shock wave device (Storz Medical).
Method: Each patient received six treatment sessions with 2,400 impulses per session on the left leg (the time interval between treatments, size of the treatment area, and energy flux density of the shock waves were not provided).
Results: Photographic analyses were used; a significant improvement in skin surface was shown for more than 70 percent of the patients. However, treatment success was not expressed according to changes in cellulite grades.
Anghern et al (2007) treated 21 patients with cellulite (grade 1, n=5; grade 2, n=6; grade 3, n=10) using defocused shock waves generated with the electrohydraulic ActiVitor-Derma® device (SwiTech Medical, Kreuzlingen, Germany).
Method: 12 sessions at intervals of 3–4 days, treatment of the skin of the lateral left and right thigh with 4,000 impulses per thigh per treatment session, homogeneously distributed over an area of 160 cm2 per side with an energy flux density of 0.018 mJ/mm2.
Results: Subjective opinion and collagenometry measurements performed with the high-resolution ultrasound system. Two patients were worse, five patients showed some worsening, two patients showed no change, eight patients showed improvement, and four patients showed clear improvement. Seventeen of the 21 patients (81%) subjectively assessed their outcome as improved. The authors concluded that their results provided evidence that low-energy defocused ESWT caused remodeling of the collagen within the dermis of the tested region.
Christ et al (2008, 2008) treated 59 patients with cellulite grade 2 or 3 with planar or radial shock waves generated with the electromagnetic Cellactor® SC1 device (Storz Medical).
Methods: The patients were split into 2 groups. Group 1 received planar shock waves generated with the C-Actor hand piece of the Cellactor SC1 device (six treatment sessions at intervals of 3–4 days, total of 3,200 impulses per treatment session with an energy flux density of 0.25 mJ/mm2 over a total area of 20×30 cm). Group 2 treated identically but with eight treatment sessions.
Results: Skin elasticity measured with the DermaLab® device and the structure of the connective tissue in the dermis evaluated with the DermaScan® ultrasound device (Cortex Technology) before and after treatment. The mean skin elasticity in group 1 patients was improved by 46% after treatment and by 78% at 3-month follow-up compared with baseline. In group 2, the mean improvement in skin elasticity was 72% after treatment, 95% at 3-month follow-up, and 105% at 6 months after baseline. The structure of the connective tissue also improved between baseline and the 6-month follow-up.
Sattler et al (2008) compared three treatments for cellulite.
Methods: Group 1 was treated with radial shock waves generated with the ballistic D-Actor 200 device (a mean of 6.2 treatment sessions, an average of 1,909 impulses per treatment session; device operated at 2.4–3.0 bar and a frequency of 15 Hz). Group 2 was treated with planar shock waves generated with the C-Actor hand piece of the electromagnetic Cellactor SC1 (a mean of 6.1 treatment sessions, 1,000 impulses per treatment session with an energy flux density of 0.35 mJ/mm2). Group 3 were treated with a combined radial and planar shock wave protocol (a mean of 6.4 treatment sessions; 2,350 radial pulses on average followed by an average of 1,925 planar impulses per treatment session; radial impulses generated by operating the control unit at 2.6–3.0 bar; planar impulses with an energy flux density of 0.35 mJ/mm2).
Results: Photographs, patient satisfaction, and skin elasticity (measured with the DermaLab device) 3 months after the last treatment session compared with baseline. Patients in group 1 had the best result. Analysis of the photographs showed an optimum treatment result for five (46%) patients, a satisfactory treatment result for three (27%) patients, and a not significant treatment result for three (27%) patients (specific criteria for optimum, satisfactory, and not significant were not specified). For patients in groups 2 and 3, the corresponding data were: an optimum treatment result in 1/9 (11%) and 2/7 (29%) respectively; a satisfactory result in 5/9 (56%) and 4/7 (57%) respectively; and a not significant result in 3/9 (33%) and 1/7 (14%) respectively. A statistical analysis was not performed. It is of note that the authors did not recognise any change in skin elasticity as a result of shock wave treatment (mean data for group 1, 11.6 mPa at baseline, 10.0 mPa after treatment, and 10.1 mPa at 3 month follow-up; mean data for group 2, 12.1 mPa at baseline, 10.8 mPa after treatment, and 12.1 mPa at 3 month follow-up; mean data for group 3, 10.3 mPa at baseline, 10.4 after treatment, and 10.9 at 3 month follow-up). The authors concluded that treatment with radial shockwave was the best choice.
Adatto et al (2010) treated 25 women on one leg each.
Methods: Ballistic D-Actor 200 device (a mean of six treatment sessions within 4 weeks with an average of 3,000 impulses per treatment session; device operated at 2.6–3.6 bar and with a frequency of 15 Hz).
Results: Comparison of the treated leg with the untreated leg 1 week and 12 weeks after the last treatment. The evaluation was performed with measurements of skin elasticity using the DermaLab device. Furthermore, three-dimensional images of the skin structure were recorded using the DermaTOP® system (Eotech, Paris, France). They found that skin elasticity, roughness elevation, and skin depression improved in a statistically significant manner on the treated legs compared with the untreated legs. They concluded that the D-Actor 200 device can be used effectively to treat cellulite without any side effects.
Russe-Wilflingseder et al (2013) randomly assigned 16 women to two groups.
Methods: Group 1 radial shock waves using the D-Actor 200 device (eight treatments once a week; 1,000 impulses at 2–3 bar air pressure applied using a DI15 deep impact transmitter then 2,500 impulses at 3–5 bar applied by the D-Actor transmitter D20-S; frequency of shock waves not provided). Group 2 sham treatment (treatment protocol identical to the RSWT protocol but using a placebo hand piece that did not emit shock waves).
Results: Clinical outcome was assessed by a patient satisfaction questionnaire, weight control, measurements of thigh circumference, visual appearance of the skin in standardised photographs, and an analysis of images taken with a specially designed three-dimensional imaging system. Patients were investigated at baseline, before the last treatment, and at 1 and 3 months after the last treatment. Statistical analysis combining the 4 measures showed significant improvement in the skin of women treated with radial shock waves but not for those treated with placebo. The authors concluded that radial shock wave treatment is safe and efficient for patients with cellulite.